Home
A Broad Introduction
Allergy Concepts
Food Issues
Asthma
Rhinitis & Hay Fever
Eczema
Children & Infants
Allergy to Animals
Finding Answers



|
Was this the answer
to the dust mite problem?
Introduction
 It is obvious that anything which will kill mites without
undesirable effects on patients could be a popular and effective way
to deal with the ubiquitous dust mite, because avoidance of the most
important allergen world-wide is so often difficult, expensive, or
impossible. From 1988 to 1994 I personally conducted clinical trials
of a German product called Acarosan which contains benzyl benzoate
to kill the mites, plus a mixture of detergents to make the mite
faeces stick together, and is presented either as a spray or a
powder which is applied to bedding, carpets, and soft furniture. My
trials were remarkably effective but the results are not acceptable
for publication because nowadays all trials have to be carried out
on a double blind basis, when neither doctor nor patient know if the
material they are using contains the active agent or an inactive
placebo. It is obvious that anything which will kill mites without
undesirable effects on patients could be a popular and effective way
to deal with the ubiquitous dust mite, because avoidance of the most
important allergen world-wide is so often difficult, expensive, or
impossible. From 1988 to 1994 I personally conducted clinical trials
of a German product called Acarosan which contains benzyl benzoate
to kill the mites, plus a mixture of detergents to make the mite
faeces stick together, and is presented either as a spray or a
powder which is applied to bedding, carpets, and soft furniture. My
trials were remarkably effective but the results are not acceptable
for publication because nowadays all trials have to be carried out
on a double blind basis, when neither doctor nor patient know if the
material they are using contains the active agent or an inactive
placebo.
Double blind trials to assess the effectiveness of a remedy are
ideally suited to testing a new drug, but when applied to an
acaricide for killing mites creates difficulties which resulted in
several inconclusive publications. The reason may be that the
patients chosen were not selected in pairs carefully
matched for their sensitivity to mites and the severity of their
allergies before being allocated to the placebo group or the active
group of patients. Without this precaution, which has not to my
knowledge been applied in any trial, it would be easy to introduce
unintentional mismatch in the severity of asthma, rhinitis, or
eczema in the two groups of patients, and seriously distort the
result. Also, no double blind placebo controlled clinical trial
could last for from one to five years, as mine did!
I have had one paper published in an American Journal, and presented
the results by lectures by detailed posters at Allergy Society
meetings in the UK, Europe, and the USA. In spite of all this
publicity within the profession I have found little or no interest
amongst colleagues in Britain, which I find difficult to understand.
Other Acaricides available here in supermarkets have never been
assessed in any sort of trials, and I have never had any good
reports
One might imagine that in spite of medical disinterest Acarosan
would have become popular and widely used. However marketing was
initially limited to clinics because the active principle is Benzyl
Benzoate, and the Health and Safety Executive (HSE) were concerned
about possible toxicity of this substance. The HSE made repeated
demands for many very expensive toxicity tests which did not make
sense because Benzyl Benzoate had been passed as safe for use in
food in the USA in 1965, had been approved in Europe to a
recommended daily intake of up to 5mg per kilo body weight in 1970,
and finally by our Ministry of Agriculture Fisheries and Food (MAFF)
in 1978.
By the time the HSE
granted full approval five years later the vendors, who had spent a
great deal of money satisfying the requirements of the HSE, had lost
interest in marketing the product. Acarosan also fell foul of the
Food and Drug Administration in the USA for the same reasons, and
sales in the USA were prohibited. Unfortunately no other company
wanted to market it, so it has not been available in the UK since
1994, but could be obtained from Germany, where Social security paid
for Acarosan until recently, when it was withdrawn because of lack
of proof of efficacy.
 At one time it was hoped that when Acarosan had been shown to be an
effective mite killer it would become prescribable by the NHS as a
method of dealing with the mite allergy problem. Benzoate has again
been banned in Europe because of safety concerns and its cost was
reimbursed in Germany for many years. At one time it was hoped that when Acarosan had been shown to be an
effective mite killer it would become prescribable by the NHS as a
method of dealing with the mite allergy problem. Benzoate has again
been banned in Europe because of safety concerns and its cost was
reimbursed in Germany for many years.
The concept of
treating the home of the patient with Acarosan instead of treating
some of the inhabitants of the house with expensive drugs seemed to
make sense, and might have saved many millions of pounds from the
NHS drug bill. Unfortunately there seems to be no possibility that
this would ever happen here, where expensive drugs are routinely
accepted as the only treatment.
This lack of interest seems surprising because, since desensitising
injections became forbidden in the UK nearly twenty years ago, no
specific and potentially curative treatment has been available for
mite allergic patients in this country, which probably has the
highest incidence of mite allergy in the world. Avoidance of the
ubiquitous mite, which is practically impossible to eradicate, is
the obvious answer. Some double blind trials have found in favour of
very expensive mattress and pillow covers, so they are often
recommended.
The first time I reported the remarkable results I was
obtaining with Acarosan at a British Allergy Society Meeting a
medically qualified person, who works for a drug company, said to my
wife at dinner that evening “I do not understand why your husband
wants to kill our best friends” A revealing remark?
My long experience with Acarosan has convinced me that it is really
effective, and that mismatch of the groups in the double blind
trials is the reason why they were inconclusive. I now present my
results using the patients as their own controls, hoping to
stimulate interest in this approach to the world wide problem of
dust mite allergy. This appears to be a practical, non toxic, and
relatively inexpensive approach to the problem, but in meanwhile the
Pharmaceutical Industry and the manufacturers of bedcovers will
continue to thrive. I must declare that I have no financial or other
interest in the promotion or sale of Acarosan, and that I was not
paid for the clinical trial.
To the practising physician the dust mite problem presents great
difficulties in management. Total avoidance by relocation to a high
dry climate, such as Switzerland where the mites cannot thrive, is
rarely possible. Very few patients are willing to throw out their
fitted carpets, soft upholstered furniture, duvets, blankets, and
pillows and put up with bare boards, linoleum, tiles, or (more
recently) laminated floors--- and perhaps also get rid of their pets
who have become part of the family. All this especially if there is
no guarantee that these extreme and expensive measures will be
effective.
 The major source of mite allergen is the bed and mattress, where
every night we supply warmth, humidity, and skin scales from our
bodies as mite food. In their turn the mites produce the faecal
pellets which are the source of the major allergen. Special
mattress covers are too expensive for impoverished patients in bad
housing conditions who are most in need of them. Quality of covers
is variable and the mattress is not the only source of mites, which
can make themselves a home in any sofa, and in the depths of the
fitted carpet. Measures to reduce the humidity to a level which will
inhibit the multiplication of the mites are neither comfortable nor
practical and very expensive. The major source of mite allergen is the bed and mattress, where
every night we supply warmth, humidity, and skin scales from our
bodies as mite food. In their turn the mites produce the faecal
pellets which are the source of the major allergen. Special
mattress covers are too expensive for impoverished patients in bad
housing conditions who are most in need of them. Quality of covers
is variable and the mattress is not the only source of mites, which
can make themselves a home in any sofa, and in the depths of the
fitted carpet. Measures to reduce the humidity to a level which will
inhibit the multiplication of the mites are neither comfortable nor
practical and very expensive.
It is obvious that the only sensible solution is to apply an
acaricide to kill them off as often as necessary, but no double
blind trials have produced a clear result, probably due to mismatch
in the severity of the allergy in the two groups. This failure to
produce a clear result, plus the regulatory authorities anxieties
about the toxicity of a spray or a powder containing a substance
allowed in many soft drinks, has had the effect of discouraging the
use of acaricides. If the acaricides contained potent insecticides,
such as are contained in ordinary fly sprays which are used
frequently in many homes, then it would make sense to be cautious.
 A recent and very comprehensive European review of the effectiveness
of the many methods of control of mite and pet allergies reached the
conclusion that there was little evidence to support the use of any
physical or chemical methods of control of dust mites or pet
allergens, based on published double blind placebo controlled
trials. This result clearly suggests that in this country dependence
on drugs is total, and that attempting to control mites is a waste
of money. A recent and very comprehensive European review of the effectiveness
of the many methods of control of mite and pet allergies reached the
conclusion that there was little evidence to support the use of any
physical or chemical methods of control of dust mites or pet
allergens, based on published double blind placebo controlled
trials. This result clearly suggests that in this country dependence
on drugs is total, and that attempting to control mites is a waste
of money.
Patients often require medication for life to control the effects of
the mite faecal particles in their environment. This is because
attempts to control mite infestation are relatively ineffective, and
the mite can produce up to 200 times its own weight of faeces in its
life-time. The full scientific name for the species of mite
commonest in England is Dermatophagoides Pteronyssinus, and the
faeces contain the major allergen, which is referred to as Der P1.
Several other allergens contained in the mite and its products have
been isolated since 1994, but Der P1 is the most important, and
measurement of Der P1 in house-dust gives an accurate assessment of
the extent of mite infestation
So, should we just give up trying to control the allergens in the
environment, and depend entirely on suppressive drugs? In my opinion
this would be to accept that we must await the day when it will be
possible to stop patients reacting to environmental allergens by
desensitising them. This could be accomplished either by the
time-honoured method of injections of gradually increasing doses of
allergen in common use everywhere in the world except the UK, or
perhaps by using the self-administered sublingual method of
desensitisation against mites which has
been established to be free from risk by double blind trials in
Europe. Modified allergens treated to
make any reactions to injections much less likely have recently been
developed and subjected to successful trials in Europe, and offer
another possibility. Unfortunately it is likely that introduction of
self-administered SLIT for desensitisation against mites will take
many years because of the restrictions imposed on clinical trials in
this country.

 The Clinical trial of Acarosan The Clinical trial of Acarosan
I will now present a brief account of the clinical trial from 1988
to 1993, based on poster presentations and talks given at Allergy
Society meetings in the UK, Switzerland, and the USA. None of these
presentations attracted any interest, and the product has been
unobtainable in the UK since 1994. This account of the trial is
presented in a narrative fashion so that it may not present any
difficulties for the reader.
80 patients were involved in the trial for periods of from one to
five years. Half of them were already well known because they had
been seen regularly by me for from 2 to 17 years. They had all been
investigated in depth and in detail, and all were dependent on
suppressive drugs for symptom control. 33 were allergic to mites
only, and the rest had multiple sensitivities. The group were
typical of any allergy clinic dealing with allergies affecting any
part of the body.
The results were assessed by symptoms diaries kept by the patients,
and daily peak flow measurements in asthmatics. At regular intervals
the amount of mite allergen in samples of house dust was measured by
a colleague who did not know the origin of the samples. I also
assessed. the amount of mite in the dust by the size of skin test
reactions to extracts of the dust samples which patients brought to
each consultation.
These patients acted as their own controls by comparing their
clinical symptoms charts, the amounts of mite allergen in the dust
from their beds, and the size of skin test reactions to extracts of
their own dust, for some time before and at intervals after using
Acarosan. One application was found to be effective for as long as a
year, probably because it has been shown that the mites eat their
own faeces, thus recycling the Benzyl Benzoate and prolonging its
effectiveness.
Assessment of the patients status took account of all body systems
involved, need for medication, and peak flow charts for asthmatics.
Special attention was paid to other factors such as pets and food
allergies or intolerances. At every visit samples of general
house-dust and bed dust were submitted, and used to make 10%
weight/volume extracts for skin testing as described elsewhere on
this website. These dust extracts were used for prick skin testing,
using Morrow-Brown Standardised skin test needles, for comparison
with the reaction to a standardised dust mite extract. The wheals
produced by the skin test reactions were outlined with biro, and
transferred to the records using document repair tape. The amount of
Der P1 mite allergen in the dust extracts was measured by Dr Terry
Merrett, using monoclonal antibodies donated by Professor Martin
Chapman of Charlottesville USA.
Once a satisfactory baseline of symptoms and treatment had been
established a supply of Acarosan was issued with full instructions
and a video on its use on bedding, mattress, carpets, and soft
furniture. No other methods to control mites were used, and no
change in cleaning routines was suggested. Acarosan was not used
again until there was evidence that further application was
necessary, as shown by Der P1 assay, skin tests using extracts of
patient’s own dust, or increasing symptoms.
|
|
|
|
Average
Levels of Der P1 at Intervals
After Applying Acarosan
|
Mean
Diameters of Prick Test Reactions to 10% w/v
Extracts of Patients Dust Samples
Average weal to Pharmacia D. Pteronyssinus was 10.3mm
(16mm -6mm)
|
  It
was very surprising that the effects of one application of
Acarosan lasted so long. It
was very surprising that the effects of one application of
Acarosan lasted so long.
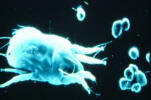
The explanation was that they eat their own
faeces, thus recycling the benzyl benzoate which kills them off.
On
the left is a video still donated by Dr J Rees where a mite is seen
with a faecal pellet in its jaws.
On the right a fluorescent dye was attached to the benzyl benzoate
so that is could be seen under fluorescent light.
The tagged
benzoate is easily seen in the gut of the mite.
Illustrative Case Histories
The results of the trial will be discussed at the end of this
section, but the story of Acarosan is best told as a narrative as
far as possible, with details of remarkable cases to illustrate
various important points
John was 19, and was first seen when he was three with rhinitis,
asthma, and eczema due to dust mite, dogs, and horses. By 1988
control was becoming more difficult, with increased sneezing,
blockage, itchy eyes, itchy palate and ears, and eczema. Three days
after treating bedroom and living room with Acarosan these symptoms
all disappeared and no treatment was required for the first time in
16 years. A month later exposure to a dirty old motor coach and an
unclean foreign hotel caused a temporary relapse of all the
symptoms, including the eczema, as shown by his excellent charts.

This unexpected challenge emphasised the dominance of the mite
allergen in all his complaints. On return home he had no problems
for 11 months, when a recurrence of his symptoms was associated with
an increase in the skin reaction to an extract of his own dust, and
in the Der P1 assay, so more Acarosan was issued. He then remained
symptom free for another three years when he had a slight relapse of
the rhinitis and the eczema, which cleared after using acarosan on
his surroundings. By 1992 he was at college, had ceased to need
inhaled steroids, and was active in sport without asthma.
Allan was 46 when he joined the trial in 1991 with a history of
asthma and rhinitis since age 17 well controlled with Becotide and
Ventolin inhalers and an average Peak flow of 405l/min. His son
David aged 13 had had asthma and rhinitis for 5 years, effectively
suppressed with the same medication, and an average peak flow of
365l/min, but exercise induced asthma prevented him playing any
games. In both father and son skin tests were markedly positive for
mites, and both had RAST 4+ for mites.
After the house was treated with Acarosan father’s peak flow rate
did not increase and he needed the same medication, as repeated
efforts to reduce medication were ineffectual, but exposure to dust
in the house did not affect him as it had done previously. Treatment
of the house had a striking effect on son David, as within two
months he was able to stop all treatment except for an occasional
puff of Ventolin, and he could play sport with no exercise asthma.
After a year his average peak flow was 364 without any treatment at
all, and he.has remained free from asthma ever since. After two
years he entered for the 1500 metres at the school sports, and then
discovered that he had left his ventolin inhaler at home. He did not
panic, and won the race without even a wheeze.
His elder brother had no allergy problems so his room was not
treated until he complained that mites were crawling across the
viewfinder of his new camera, and he captured a few which were
identified as Lepidoglyphus destructor, the species of mite which is
usually found on farms. The dust from his room assayed very high,
and an extract of his room dust produced a reaction on his father’s
skin 17 mm in diameter, but produced none at all on his own skin as
he was not an allergic person. The reason for the infestation was
that he ate biscuits when studying, and destructor loves to live on
cereal., so his room was also decontaminated.
David has continued to be free from asthma and is now aged 29. Until
age 19 both skin and blood tests remained very positive without
symptoms to match, while the assay of his dust remained very high,.
a finding which could have been very confusing. Clearly he had
adapted successfully and no longer reacted to mites, perhaps because
a window of a relatively mite free environment had been created for
a few years. He seems to be a definite cure.
Father Allan also recovered, as five years later he had stopped his
Becotide and his peak flow rates were 455, but the skin tests were
still very positive. Ten years later he is well on inhaled treatment
only.
A very serious Eczema problem
 Stephen was 29, and had had eczema for three years which was so
severe that three different dermatologists could offer no
alternative except indefinite oral steroids and steroid creams. When
first seen he had severe generalised weeping eczema, was almost
suicidal, and was taking 10 mgms of prednisolone daily. Prick skin
tests were very positive for mites, and also to an extract of his
own bed dust, which assayed at 229 micrograms of Der P1. This is
very high, as 5-10 micrograms is unacceptable in the home of a mite
allergic patient. Following the use of Acarosan in bed, bedroom, and
living room he was able to stop oral steroids and was about 80%
improved in a month. Stephen was 29, and had had eczema for three years which was so
severe that three different dermatologists could offer no
alternative except indefinite oral steroids and steroid creams. When
first seen he had severe generalised weeping eczema, was almost
suicidal, and was taking 10 mgms of prednisolone daily. Prick skin
tests were very positive for mites, and also to an extract of his
own bed dust, which assayed at 229 micrograms of Der P1. This is
very high, as 5-10 micrograms is unacceptable in the home of a mite
allergic patient. Following the use of Acarosan in bed, bedroom, and
living room he was able to stop oral steroids and was about 80%
improved in a month.
By 3 months he had cleared completely, and
remained clear without any treatment until he spent a weekend in a
dirty and dusty flat. After the first night he began to itch, and
after the second night he had a severe relapse of the eczema lasting
two weeks and requiring a course of oral steroids. During the next
two years the eczema cleared up completely, in spite of the fact
that the amount of Der P1 in the dust increased to 33 micrograms,
and his brother developed asthma due to mites.
His eczema did not
relapse until the Der P1 reached 98.5 in November 1991, cleared
after using Acarosan, and relapsed again in 1992 when the Der p1
reached 133 micrograms, but cleared in two weeks after Acarosan.
Subsequent follow-up to 1995 revealed that slight relapses occurred
every year which were abolished by using Acarosan. Further contact
has been lost.
An Eczematous Family Affair
 Alan aged 29 and his two daughters aged 21/2 and 4 years all had
eczema. The younger child cleared completely on avoiding egg, but
the elder child had a big skin reaction to mite, and also to a
family dust extract, which assayed at 28 micrograms of Der P1. At
first another acricide (Allerex) was applied, but after using no
less than 4 litres there was only slight improvement in the eczema
and in the skin reaction to the family dust extract, but the assay
was down to 5 micrograms. Acarosan was then introduced, and after 6
weeks there was no skin reaction to the family dust extract, which
assayed at 2,2 mcgms, Father’s life-long eczema subsided, his hands
were clear for the first time in his life, and daughter cleared
completely. The skin tests shown were carried out on the father’s
skin. A few months later a new wool carpet was laid. After six weeks
eczema recurred on the child’s knees, but cleared after acarosan was
applied to the new carpet, suggesting that it had become colonised
by mites in that short time. Alan aged 29 and his two daughters aged 21/2 and 4 years all had
eczema. The younger child cleared completely on avoiding egg, but
the elder child had a big skin reaction to mite, and also to a
family dust extract, which assayed at 28 micrograms of Der P1. At
first another acricide (Allerex) was applied, but after using no
less than 4 litres there was only slight improvement in the eczema
and in the skin reaction to the family dust extract, but the assay
was down to 5 micrograms. Acarosan was then introduced, and after 6
weeks there was no skin reaction to the family dust extract, which
assayed at 2,2 mcgms, Father’s life-long eczema subsided, his hands
were clear for the first time in his life, and daughter cleared
completely. The skin tests shown were carried out on the father’s
skin. A few months later a new wool carpet was laid. After six weeks
eczema recurred on the child’s knees, but cleared after acarosan was
applied to the new carpet, suggesting that it had become colonised
by mites in that short time.
One year later the family moved to a completely renovated old house
with more space, taking with them all the treated carpets and
furniture. Within four months the elder child’s eczema was
reappearing, and she had her first asthma arrack. Her sister aged 2,
whose eczema had previously disappeared after avoiding egg, now
developed slight eczema. The assay of the Der P1 in the house dust
of their new house was found to be 24 micrograms, nearly as high as
the first assay before the previous house was treated. Skin testing
revealed that she had now become positive to both mite extract and
to bed dust extract, yet she had been negative only a year before.
With liberal use of Acarosan the itching, scratching, and eczema
cleared up, and three years later eczema had not recurred in any
member of this family. This family affair shows how closely mite
infestation can be related to the eczematous reactions of a family
living in a Victorian house with more accommodation which must have
had an unseen and unsuspected population of mites which re-infected
their bedding, furniture, and carpets, previously treated with
Acarosan.
A long-standing case of eczema
|
Mary was first seen aged 26 with severe hand eczema, due to dust
mite and was carefully desensitised with considerable improvement
for five years, but slowly deteriorated until seen again aged 44.
She had been hoovering her five year old mattress regularly
every few weeks as
instructed.
The skin test reaction to the standard mite extract was
12mm across, but to her own dust extract it was 17mm, with a severe
delayed reaction the next day.
Her dust was found to be loaded with
faecal particles in spite of the fact that another acaricide,
Actomite, had been used on bed and bedding a month before, and the Der P1 assay was very high at 312 micrograms.
The microphotographs
show the remarkable decrease in faecal particles after only 21 days
and in the skin test reaction.
Further follow-up was not possible |
 |
 |
|
|
|
|

Skin reaction to dust extract after 21 days using Acarosan |
A Mite Infested House can cause Severe Eczema
Mark was 35 and had had mild eczema since infancy, as had mother and
brother. Four dermatologists had been consulted at various times.
One did patch tests which showed nickel sensitivity, but none did
skin prick tests. He had been much worse since purchasing an old
damp house and spending much time renovating it. A local
dermatologist had admitted him to hospital twice, and he had had
oral steroids several times in the previous year.. The only
occasions when he had been better was when camping, or when in
hospital for a week without treatment, only to relapse within two
days on return home.
When seen he had very severe weeping eczema requiring oral steroids
for control. Prick skin tests were +++++ for two species of mite and
for his own dust extracts. His Total IgE was the highest ever seen
at 43,000 units ( normal maximum about 100) with specific IgE ++++
for 5 species of mite. He saw mites crawling on a black surface, and
captured some for identification. Attempts to control the
infestation with acarosan were relatively ineffective, which was not
surprising because the previous owners had covered many walls with
polythene and stuck wallpaper on top, the whole acting like blotting
paper in damp areas Four months later he moved to a modern flat with
new carpets and furniture. He stopped itching in a week, and the
eczema was negligible by three weeks. In this case the infestation
was so bad that the acaricide could not control it. The lesson is
that anyone with mild eczema would be unwise to buy an old house,
especially if damp.
Asthma and Rhinitis
Deborah was first seen aged 17 with asthma for 3 years due to mites
and was successfully desensitised, but 12 years later, after
injections for asthma were forbidden, she relapsed and became
difficult to control requiring frequent courses of oral steroids.
Her bed dust assayed at 199 micrograms of Der P1, but after
Acarosan was applied all treatment ceased. The only exception was
that when she visited her parents, who had an old dusty house, she
always reacted with sneezing and wheezing. She has remained easily
controlled even after Acarosan became unobtainable
Andrew was aged 15 with severe asthma and rhinitis controlled with
steroid inhalers and bronchodilators, peak flow average 450. Three
months after using Acarosan all treatment ceased without relapse,
peak flow averaged 500, all symptoms were absent for the first time
In 5 years, and he was able to play football without asthma.
Acarosan was used for two years only. The only time he had an attack
of asthma was after attending a concert in an old theatre, and after
accidental exposure to a dust sample in my consulting room ! His
mother was also a dust allergic. She had wheezed every night for 14
years, but ceased after Acarosan was used.
The Der P1 assay in his bed was 179 micrograms to begin with,
falling to very low levels after Acarosan. Two years later he went
off to college, and neither asthma not rhinitis relapsed in dusty
students lodgings, and he was able to play football without any
problem. Aged 20 he was apparently cured of his asthma as he did not
relapse even when his bed dust contained 41 micrograms/Gm, a very
high reading well over the recognised upper limit for mite
infestation as a cause of asthma.

Summary of Results

Is Acarosan an effective answer to the mite problem?
I had been very interested in mite allergy since 1968, when I
published the first study from this country confirming that the mite
was the major allergen in house-dust, in spite of much scepticism at
that time. The story behind this trial is that when attending a
meeting in Washington D C in 1985 I heard a presentation on Acarosan
which was so interesting that I made a firm contact with the speaker
afterwards. I heard nothing more for two years, when the
manufacturers wrote asking if I could put them in touch with a
company in the UK to market their product. I made enquiries on their
behalf but found no interest whatever. They supplied me with many
copies of a video regarding the mite and Acarosan, which I sent to
prominent members of the British Allergy Society, but nobody seemed
to be interested. Finally a small pharmaceutical company agreed to
market it, and supplied enough for an open clinical trial. The
comment from an employee of a drug company after the first
presentation of my results that I was “killing their best friends”
is revealing.
The improvements correlate well with the decrease in skin tests and
allergen in the dust samples lasting for at least a year. The
persistence of the acarosan because of the nasty habits of the mites
recycling the acarosan was an unexpected finding of great
importance, as treatment of the house about once a year or when
required is much more acceptable. Recurrence of symptoms on exposure
to untreated houses, hotels, and theatres is important evidence
confirming the persistence of allergy to mites, and also confirmed
that the improvements are due to the Acarosan. Treating the house
instead of the treating the inhabitants for life with expensive
drugs is a concept which could save many millions from the NHS
budget because mites are such a common cause of allergic problems.
Improvements in asthma, rhinitis, or eczema in children living in
the same house as a patient were noted in ten instances was an
unexpected bonus which supports the concept of treating the
environment instead of the patient..
Less than half of the patients had a solitary allergy to mites, the
rest being sensitive to a range of other environmental allergens and
sometimes foods as well. Almost total abolition of mites from the
home for a prolonged period has not been achieved before, and has
enabled better understanding of the relative importance of mites,
pets, and foods in the causation of allergic disease. Results in the
more complex cases were not as good as in the 33 cases where mite
was the sole cause, emphasising the difficulties in assembling a
homogeneous group of allergic patients suitable for a double blind
placebo controlled trial, and also keeping them motivated for long
enough to get a clear result. Entrants to any trial in allergy must
be fully assessed by a clinical allergist, and ideally only pure
mite allergics accepted and sorted into matched pairs for severity
of symptoms
The results in eczema are the most dramatic and gratifying, and
confirm the importance of mites as a cause of eczema. In the face of
this evidence it is even more difficult to understand why British
dermatologists still seldom accept that allergy is a very important
cause of eczema, and are unwilling to carry out prick skin tests.
Perhaps the reason is that some departments may have facilities only
for patch testing. The remarkable potency of 10% bed dust extracts
suggests that when eczema sufferers are in bed at night, when the
itching is at its worst, mite faecal particles on the skin require
just a trace of sweat to produce a very strong mite extract which
penetrates the cracks in skin which is already damaged, causing
intense continuous skin reactions, scratching, and infection.
The most important finding by far is that in some young patients
sufficiently prolonged absence of mites in the environment
eventually brings about re-adaptation and tolerance, so that they no
longer react to untreated environments and are able to stop all
medication without relapse. This phenomenon has also been observed
in Europe in some children who have had prolonged stay at schools in
the Alps where the mites cannot survive.
It is very gratifying to have actually cured some of these allergy
victims, and it seems a great pity that this method of mite control
has not been used more widely. These results suggest that if mite
control could be used more often in children they would have a
chance of escaping from the allergic march. |