Home
A Broad Introduction
Allergy Concepts
Food Issues
Asthma
Rhinitis & Hay Fever
Eczema
Children & Infants
Allergy to Animals
Finding Answers



|
Becotide Results
1970-1980
Today it is taken for granted that asthma is treated with inhaled
steroids, and nowadays very few asthmatics are dependent on oral steroids. Some
account of the early days of the first trials may be of interest,
as this was a very exciting time leading the world in the treatment
of asthma and rhinitis. These open trials would never have been accepted for publication
nowadays, but the
results, especially in children, were so obvious that double blind
trials would really have been unnecessary and unethical.
Although
Becotide and other inhaled steroids have had a tremendous impact on
the treatment of asthma affecting both children and adults, I feel
that the very effectiveness of this therapy has made it less important to find out the causes of asthma or rhinitis.
Today the diagnosis of asthma or rhinitis is almost invariably
followed by the prescription of inhaled steroids, and very seldom by
any effort or tests to define the cause.
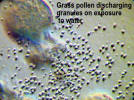
From 1958 to 1971 I had directed my main research efforts towards
Aerobiology, which involves the capture, identification, and
counting of the pollens and spores which cause seasonal hay fever
and asthma, and with effective desensitisation which is actually
curative treatment.
In fact my rescue of Becotide made it unnecessary for the doctor to
know the cause of his patient’s problem in most cases of respiratory
or nasal allergy, and rendered my aerobiology research much less
important.
Dependence on suppressive drugs for the treatment of allergy became
total when desensitisation injections became impossible from 1986. Fortunately desensitisation treatment is now being allowed by
the sub-lingual route for hay fever, but the NHS will seldom pay for
this. It will take many years to achieve the availability of this
form of treatment, used widely in the rest of the world, to be
permitted for the unfortunate allergics of this country
Improvements in Chest
Deformities
Before 1970 gross chest deformities in children were not
uncommon, and photographs were taken before and at intervals after
the introduction of Becotide show their disappearance. In adults
dependent on oral steroids, the photographs show the remarkable
changes in their facial appearance and obesity after transfer to
inhaled steroids. A selection
of unpublished pictures and peak flow charts showing dramatic
improvements are shown here as a matter of historical interest.
|
|
|
This boy
aged 14 had such unstable asthma that he
had to have frequent courses of oral
steroids
|
 |
|
When he
was started on Becotide he rapidly came
under control but is dependent on
inhaled steroid to this day. He was
repeatedly skin test negative, but a
retest aged 20 produced a +++++ reaction
to mites
|


|
This 50 year old patient had severe unstable asthma frequently
requiring emergency oral steroids. He had perfect control for the
next 34 years, and died of unrelated causes aged 84

Pauline was aged 8 in 1971, and was a very unstable multiple
allergic living on a farm as shown above by peak flow records. The
black areas at the bottom represent frequent short courses of oral steroids


It was finally decided to try her on Becotide at the end of 1971,
and her peak flow stabilised at once. She is now 48 and still
maintained on Becotide. Serial photographs were taken over the next
few years, as shown below.
On the left is a picture of Pauline aged 7, showing a very unhappy
child breathing through her mouth because the nose is blocked by
rhinitis, with the beginning of a pigeon chest, which is developed
further in the middle photo taken before she began Becotide. On the
right she is now aged 12, and the deformity has almost disappeared
after 30 months on Becotide with complete control of the asthma

|

|
This boy aged 14 had developed a chest deformity from chronic
asthma.
After a year on Becotide with complete control of his
asthma, and being able to take normal exercise and sport for the
first time the shape of the chest has become normal.
He is now aged 47 and still requires Becotide daily
|

|
John was only
two and a half when the photo on the left was taken. He had
been treated elsewhere with oral steroids for some time,
with obvious side-effects and retardation of growth.
I doubted if
we could get him to use an inhaler at his age, but with his
mother’s persistence he learnt to use an inhaler properly.
Oral steroids were stopped and he did very well as shown by
the second picture taken only a year later showing rapid
growth and disappearance of the steroid side-effects.
He developed
normally into a healthy young man, except for the asthma for
which he still has to take Becotide daily. He has been a
game keeper for some years and is now aged thirty-six.
|

|
This girl began to wheeze as
a baby, and was, treated elsewhere with oral steroids
from about age five. She had been on continuous steroids
for five years when the first photo was taken, showing
the stunted growth, moon face, and obesity typical of
steroid dependency. She was successfully transferred to
Becotide, and her average peak flow rose from an average
60 L/min to 140, (predicted peak flow was 230). The
picture 14 months later shows rapid growth of 8cms and
disappearance of the side-effects. She was eventually
able to do cross-country running and swimming, but some
years later she had to have oral steroids again. All
contact has been lost with this case.
|

|

|
Rachel was
aged 6, and a very unstable asthmatic when the photo on the
left was taken.
The photo on
the right was taken after she had been perfectly controlled
with Becotide for nearly two years.
The
difference in every way is quite remarkable. |
Becotide Results 1970-1980
|
|
|
|
The graphic presentation
on the left shows how the steroid dependent children
were much more likely to be able to transfer to
Becotide, and how the older the patients were the less
likely was transfer to Becotide to be successful
|
 |
 |
|
This group were less
severe asthmatics who had not had to be treated with
oral steroids except for a flare-up. Older patients were
only slightly more likely to have problems in becoming
stabilised on Becotide.
|

Comments
Patients treated with Becotide were all monitored using peak flow
meters, the last reviews from my clinic being in 1980. Obviously the cases
illustrated here were carefully selected to show dramatic results,
but are by no means exceptional. A series of papers from Derby were
published from 1971 to 1980, and thousands of studies from
investigators all over the world on various aspects of inhaled
steroids have been published over the years. The use of aerosol
steroids for rhinitis has also been studied in Derby and a survey
over a five year period, in which Beconase had been used in 223
patients, showed no long-term side-effects in 534 patient/years of
use.
Anxiety has lingered over the possibility that long term use would
result in adrenal suppression or osteoporosis, especially in
post-menopausal women. Several negative studies on this aspect have
been published, but have usually been for a few years only. Many
patients in the Derby group have been using Becotide for up to
forty years. No reports of serious long-term side-effects have
surfaced, so it seems most likely that no significant
side-effects occur even after so many years, but I have consistently
failed to persuade anyone to recall these patients and carry out a comprehensive
survey to settle the matter.
From about 1968 onwards all allergic patients attending the Derby
Chest Clinic had not only the usual case records, but also a punch
card system on which brief notes of each consultation were made.
Furthermore, all case notes were dictated while the patient was seen
and typed, so there is a unique legible record of each case is in
existence. When I retired from the NHS in 1982 I was not replaced by
anyone with an interest in allergy, and as a result one of the
largest allergy clinics in the UK was disbanded and most of the
patients referred back to their General Practioners. Some continuity was preserved
by the nurse specialist, and the punch card records of the trials
carefully preserved, but she has now retired. These punch card
records have now been taken over by Nottingham University and it is
hoped that the group of patients who were the first in the world to
receive inhaled steroids, and have been taking them ever since, will be reviewed This would finally demonstrate if
inhaled steroids can be used for life without fear of side-effects
or not.
|
|
|
|
|
Appearance in 1971, after
5 years on
oral steroids for asthma
|
|
One year after transfer
to Becotide.
'Slimmer of the year' 1972.
Still taking Becotide 2005.
|
|