Home
A Broad Introduction
Allergy Concepts
Food Issues
Asthma
Rhinitis & Hay Fever
Eczema
Children & Infants
Allergy to Animals
Finding Answers



|
It may help in understanding allergies to describe how a case would
be investigated in depth and in detail. The most important part of
an allergy investigation is taking a very detailed case history,
always including the family history, because if many family members
also have allergies then the patient’s problems are also more likely
to be due to allergy. Taking an allergic case-history properly is
very interactive and time-consuming, depends on the experience and
knowledge of the investigator, and is an example where art of
medicine still takes precedence over science.
 An experienced Allergist will know the correct questions to ask and
how to elicit detect significant clues in the patient’s answers
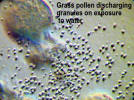
which may suggest the most likely causes. For example, if hay fever
or asthma is limited to June and July grass pollen is certainly the
cause, but if it begins in the spring tree pollens are also
involved. Symptoms continuing into the autumn, or becoming worse in
damp weather, suggest that seasonal mould spores are also involved.
Symptoms all year round suggest an allergen constantly present in
the environment. An experienced Allergist will know the correct questions to ask and
how to elicit detect significant clues in the patient’s answers
which may suggest the most likely causes. For example, if hay fever
or asthma is limited to June and July grass pollen is certainly the
cause, but if it begins in the spring tree pollens are also
involved. Symptoms continuing into the autumn, or becoming worse in
damp weather, suggest that seasonal mould spores are also involved.
Symptoms all year round suggest an allergen constantly present in
the environment.
Observant patients may have noticed important circumstantial
evidence relating to their sufferings, but may not mention their
experiences unless asked directly by the allergist because they do
not realise that their observations are important. For this reason
an experienced allergist will ask essential leading questions which
are always asked again later to check for consistency.
 Sometimes the cause of the problem is in the working environment.
For example if the patient is better at weekends, gets worse during
the week, improves on holiday, and relapses promptly on return to
work, an occupational cause is likely. Sometimes the cause of the problem is in the working environment.
For example if the patient is better at weekends, gets worse during
the week, improves on holiday, and relapses promptly on return to
work, an occupational cause is likely.
Blowing a Peak
Flow Meter several times a day can sometimes produce evidence
supporting an occupational cause. If the cause is in the home
environment the patient should be better at work than at home,
and better on holiday away from home, especially in a sunny
climate, only to relapse on return home, often by the next
morning.
The above comments refer mainly to asthma or rhinitis, but in other
complaints such as migraine, eczema, irritable bowel, ulcerative
colitis, nasal polyps, rheumatoid arthritis, behaviour problems in
children, etc there may or may not be clues in the history
suggesting that a daily food might be the cause. In eczema,
especially in children, both foods and environmental allergens such
as dust mites or pets may be involved, so all the allergens involved
have to be avoided simultaneously to obtain relief from symptoms.
Sometimes sufferers observe that their problems improve when they
are unable to eat due to a stomach upset or diarrhoea, only to recur
when they start to eat again. This can be an important observation,
but the reluctance of many medical colleagues to accept the
possibility
that food can cause many illnesses is difficult to understand.

 Skin testing Skin testing
Prick skin testing is a simple, safe,
and almost painless way to test for allergies. Skin testing can be
carried out in babies, and it is a common medical fallacy, even
amongst paediatricians, that skin tests cannot be done until five or
six years of age. Prick tests are performed by placing drops of
extracts of the most likely causes of the allergy on the skin of the
forearm or sometimes the back. The drops of test extract are then
pricked through. using my specially made sterile standardised
disposable plastic needles as illustrated. The prick tests are
almost painless, and do not cause bleeding because the point is just
the right length to reach the living cells of the skin and no
further. As the needles are identical the tests are also
standardised so that one reaction can be compared with another.
I invented these special testing needles many years ago, and
although very seldom used in this country they are popular in
Europe, USA, and Canada, Any positive reactions, which resemble an
itchy insect bite, will appear in ten minutes, and indicate the
likely causes of the allergy. In the UK, steel disposable prickers
are most often used, but are very similar.
 |
 |
 |
 |
| Morrow Brown
Test Needle |
Cat & Dog |
Cod, Tuna,
Salmon |
Peanut & Egg |
The meaning of skin test reactions
 Unfortunately, the interpretation of the results of prick skin
testing is not straightforward, because many people have latent
allergy (‘atopy’) which is not causing any symptoms but can produce
meaningless false positive skin reactions. Although it is very
convenient for the allergist that the skin all over the body becomes
specifically sensitised to allergens, this can also be confusing
when the prick test is positive but there is no history of reacting
to the allergen. Unfortunately, the interpretation of the results of prick skin
testing is not straightforward, because many people have latent
allergy (‘atopy’) which is not causing any symptoms but can produce
meaningless false positive skin reactions. Although it is very
convenient for the allergist that the skin all over the body becomes
specifically sensitised to allergens, this can also be confusing
when the prick test is positive but there is no history of reacting
to the allergen.
Skin test reactions cannot be taken at their face value, and their
significance depends on the case history and the experience of the
allergist in deciding which are the most likely possibilities.
Sometimes a test extract is not available, but can sometimes be
improvised by first sticking the needle into the suspected fruit, or
vegetable, such as an apple or a potato, and then into the skin of
the patient using the same needle, so that a tiny trace of the juice
is inserted into the skin.
Some testing extracts are more reliable and more potent than others,
and sometimes the process of making the testing extracts destroys
the allergen so it does not produce a reaction when it should.. For
example many tests for foods are useless for this reason, but egg,
fish, shellfish, lupin flour, and peanuts are reliable. Skin tests for
milk and milk proteins, and for wheat, are only sometimes positive.
Thus, although skin testing is simple, interpreting the results can
be difficult and requires much experience.
Special Tests for Environmental Possibilities
For many years I have provided a unique service by using the
patients own house dust or pet hairs to make instant extracts for
skin testing against their own environment. When the hair of a
family pet is used in this way and the result is a dramatic positive
it is much easier to convince the patient that a good home should be
found for the pet! This direct and very specific approach, not
available anywhere else as far as I am aware, can demonstrate
clearly and obviously if the cause of the allergy is in the home
environment. The major source of dust mites in the home can also be
pin-pointed.
 A good example of how helpful these tests can be is the case of
Susan who was twenty-nine when she bought an old house about 100
years old with second hand furniture, including a three piece suite
and the bed, and the old carpets. From about six weeks after moving
in she developed a rash on the arms, which became gradually worse
over the winter, and after wall-papering. A good example of how helpful these tests can be is the case of
Susan who was twenty-nine when she bought an old house about 100
years old with second hand furniture, including a three piece suite
and the bed, and the old carpets. From about six weeks after moving
in she developed a rash on the arms, which became gradually worse
over the winter, and after wall-papering.
The eczema spread to
involve the whole body by one year, more or less controlled by
steroid creams prescribed by the University Hospital Dermatology
Clinic.
During the next year she became worse despite lavish
application of steroid creams and Oilatum baths, etc and was so
itchy that she could not resist scratching, slept badly, and dreaded going to bed.
Painting her bedroom
precipitated a flare-up of her eczema so severe that she was
admitted to hospital for ten days.. She requested allergy testing,
but only patch tests were carried out, which were all negative, and
RAST blood test which showed only a slight positive for cat, but
”not enough to justify getting rid of the cats”. She continued under
the care of the skin clinic, living in her old house with the two
cats for the next year, when she decided to put her cats in a
cattery and live with her parents who had had a new house, but a dog
and a cat.
She improved rapidly in this environment, suggesting that the old
house was the cause, so she requested referral for allergy
investigation. I found that she had negative skin reactions to dust
mites, but was very positive to dust from the bed and the sofa, as
shown.. There were also reactions to cat, dog, and horse, all of
which she could tolerate without trouble. She remained well at her
parents new house with the cat and the dog, sold the old house, and
bought a new modern house in which she remains free from eczema but
living with two cats.
Blood tests
-
 Scientific blood tests (RAST) have been developed to help in these
dilemmas, but are not always helpful either!! Positive skin tests
mean that cells of the skin are sensitised, and that an antibody
called specific IgE is present in the blood of that particular
patient. The amount of this specific antibody in the blood as
measured by RAST, usually reported as six grades of positive, will
give some idea of the importance of IgE antibody in causing the
symptoms. Scientific blood tests (RAST) have been developed to help in these
dilemmas, but are not always helpful either!! Positive skin tests
mean that cells of the skin are sensitised, and that an antibody
called specific IgE is present in the blood of that particular
patient. The amount of this specific antibody in the blood as
measured by RAST, usually reported as six grades of positive, will
give some idea of the importance of IgE antibody in causing the
symptoms.
-
Measuring the total of all the IgE allergy antibodies ( The Total
IgE ) in the blood may also help, but can be disappointing and
confusing. For example in eczema huge amounts of IgE antibodies are
often present without any indication of which specific IgE
antibodies are important. The Total IgE in asthma may also be high,
with varying amounts of specific IgE to common allergens such as
pollen, dust mite, and pets. The amount present will suggest the
importance of each allergen in conjunction with the case-history,
and give useful information helpful in the management of the case.
However a Total IgE reading within normal limits does not exclude
allergy, as is sometimes thought, because it may conceal quite a
high positive test for specific IgE directed towards one specific
allergen which has not been tested for.
-
When the skin tests are all negative we cannot go further, unless
the most likely allergens are suggested by the history, for which
testing extracts may not be available. If the Total IgE is very
high, without any skin test reactions or history to suggest what the
important allergen may be, a specific daily food for which no test
is available is a possibility. Sometimes the story will suggest
which specific food may the cause, and pricking some of the food or
juice into the skin produces a confirmatory reaction, as in the case
of allergy to lupin flour described on another page.
It is obvious that if the cause of an allergic problem can be
identified and avoided a ‘cure’ is possible. Unfortunately this is
not easy, because even if the trigger is found it may one which is
impossible to avoid. At present there are there are laboratories
claiming that they can to find the cause of your allergy from a drop
of your blood, but the significance of the results is doubtful
because these tests have not been subjected to acceptable scientific
trials. Many complementary treatments are advertised which have
never been proved to be either significant or effective, so you have
been warned.. There is no quick fix.
Cytology tests (Microscopic examination of cells from the patient)
In 1958 I discovered that if microscopic examination of the
sputum from an asthmatic patient revealed many eosinophil cells
typical of an allergic reaction, I could confidently predict that
oral steroids would be dramatically effective. Although this test
indicates the most effective treatment, it does not identify the cause.
When these eosinophil cells are not present oral steroids are
unlikely to be very helpful. This finding became even more important
in 1970, when this same test enabled me to select proven
allergic asthmatics for the first successful clinical trials of Becotide, the very first steroid aerosol. Trials elsewhere had shown
the aerosol to be ineffective, and the makers were on the point of
discarding it as useless, but. trials in Derby showed that in
proven asthmatics the aerosol was very effective indeed, so the
manufacturers decided to give the drug another chance. Before long
inhaled steroids were used world-wide, and this treatment
acknowledged as the most important advance in asthma therapy in the
last 30 years because inhaled steroids control most asthmatics
without the long-term side-effects caused by oral steroids.
Examination of a smear of the nasal mucus is equally helpful in
chronic rhinitis to decide if it is allergic or not and whether
nasal steroid sprays will help. Cytological examinations carried out
during a consultation enable correct decisions regarding the most
appropriate treatment to be made on the spot, regardless of the
presence or absence of skin test reactions. I am not aware of anyone
else in Britain who does this investigation right there in the
consulting room.
 |
 |
| Macrophages
in bronchitis |
Eosinophils in allergic asthma or rhinitis |

This patient is unique. His response to steroids changed many times
over the years,
according to whether eosinophils were present or not
Bronchial and Nasal Provocation Tests
A bronchial provocation test is a carefully controlled exposure by
inhaling an aerosol of a dilute solution of the suspect allergen.
This will produce a slight attack of asthma if the allergen used is
the cause. Many years ago I devised a method of carrying out this
test safely, and in such a way that an answer was obtained without
causing a severe attack of asthma. Nasal provocation tests can also
be done to find the cause of chronic rhinitis by placing a drop of
test extract in the nostril..
 Before 1986 this procedure was routinely used in my clinic order to
prove the cause of the asthma, and to prove that desensitising
injections, (referred to today as immunotherapy) were necessary.
After a course of desensitising injections containing this allergen
in gradually increasing amounts had been completed another
provocation test would be carried out to show if the treatment had
made the patient immune to the allergen or not. If still positive
further injections were given until the provocation test became
negative. This regime was very successful in many asthmatics, with
lasting results which will be shown elsewhere in this website, but
only as a matter of interest.. Before 1986 this procedure was routinely used in my clinic order to
prove the cause of the asthma, and to prove that desensitising
injections, (referred to today as immunotherapy) were necessary.
After a course of desensitising injections containing this allergen
in gradually increasing amounts had been completed another
provocation test would be carried out to show if the treatment had
made the patient immune to the allergen or not. If still positive
further injections were given until the provocation test became
negative. This regime was very successful in many asthmatics, with
lasting results which will be shown elsewhere in this website, but
only as a matter of interest..
Today it is unreasonable to subject a patient to a provocation test
to prove the cause of their asthma because, since 1986, we cannot follow up a positive reaction with injection
treatment to desensitise them against the allergen involved. The
only justification for a provocation test nowadays would be to
confirm that the cause was something which could be totally avoided
or removed.
An over-reaction by the Committee for Safety of Medicines in 1986 is
still preventing the effective treatment of inhalant allergies in
this country. Timidity rules OK today, so we have to practise
defensive medicine, watch our backs, and deprive our patients of
potentially curative treatment.! Desensitisation by using drops
taken daily under the tongue by the patient at home instead of
injections has been shown repeatedly in Europe and elsewhere to be
safe, and is now permitted in the UK, but the NHS nearly always
refuse to pay for this treatment. Details of my successful
unpublished trial of
sub-lingual treatment twenty years ago are
given elsewhere in this website.
Challenge Tests for Food Allergies
Skin tests and blood tests for foods are often unreliable, so the
only test which really proves a food allergy is to eat it and
observe what happens. When the patient is allergic to a food great
care is necessary because a tiny amount may trigger off a serious
reaction, so never do a test yourself if there is an question of an
allergy to a food because it can be dangerous.
For example after
avoiding peanuts with great care for years it may be questioned if
the allergy has subsided, but a deliberate challenge by feeding a
small amount is the only way to be certain. Food challenge for foods
such as peanut must always be carried out in hospital with emergency
equipment at hand in case of a serious reaction. Challenge tests may
also be carried out double blind to prove beyond all doubt if it is
still necessary to avoid peanut or other potent allergens with great
care.
Challenge Tests for Diagnosis of Food Intolerance
 Patients suffering from food intolerance are quite different because
normal amounts of food are needed to cause a reaction which is often
delayed by up to 24 hours, sometimes even longer. Challenge tests
can be done at home because the effects are not so severe, sudden,
or potentially dangerous as in food allergy, but should be carried
out only when asked to do so. Challenge tests using suspect foods
are very necessary, but usually carried out only after removal of
the main possibilities from an elimination diet has brought about
obvious improvement Obviously if there is only a short interval
between eating the food and the onset of the effects, and it happens
every time, that food must be avoided completely. Patients suffering from food intolerance are quite different because
normal amounts of food are needed to cause a reaction which is often
delayed by up to 24 hours, sometimes even longer. Challenge tests
can be done at home because the effects are not so severe, sudden,
or potentially dangerous as in food allergy, but should be carried
out only when asked to do so. Challenge tests using suspect foods
are very necessary, but usually carried out only after removal of
the main possibilities from an elimination diet has brought about
obvious improvement Obviously if there is only a short interval
between eating the food and the onset of the effects, and it happens
every time, that food must be avoided completely.
Ideally, food tests should be double blind, but being given the
offending food by mistake, or in a restaurant, can be very
convincing. In clinical practice open testing for food intolerance
is the only practical method, but with the cooperation of a partner
a single blind test is possible. Whatever method is used it is
important to demonstrate that the same amount of food causes the
same effect after the same time interval, preferentially on three
occasions.
 Demonstrable repeatability is necessary because it is so
easy to jump to conclusions and end up with a restricted diet for no
good reason. To discover the causes and avoid them has the
potential to improve quality of life and greatly reduce the need for
medication. Demonstrable repeatability is necessary because it is so
easy to jump to conclusions and end up with a restricted diet for no
good reason. To discover the causes and avoid them has the
potential to improve quality of life and greatly reduce the need for
medication.
A careful food diary which notes everything that passes the lips,
including medicines, vitamins, supplements, sweets, and even
toothpaste, is an essential part of tracking down the causes of a problem, whatever it may be.
Only in this way is it
possible to spot a delayed reaction to something eaten the day
before. If the cause is a daily food it is obvious that symptoms
should be fairly constant, and that only by using elimination diets
will it be possible to make sense of the problem. |